



Clitoris correction - Correction of the clitoris and clitoral hood
Clitoris means "small hill", and for most women it is very sensitive and responsive to sexual stimulation. Up to 8000 nerves end here. It is the only organ in the human body that serves exclusively for sexual stimulation. The anatomy of the clitoris corresponds to that of the penis. Anomalies in size and shape can mainly be caused by hormonal influences during embryonic development.
True enlargement of the clitoris (clitoral hypertrophy) is very rare and is often confused with enlargement of the clitoral hood (preputial hyperplasia) or a visibly protruding clitoris (clitoral protrusion).
The clitoris has a three-dimensional structure in the shape of an inverted Y, with the two arms lying on the pubic bone. The fusion of these two arms develops into the clitoral shaft, which is also found lying deeply over the pubic symphysis. The tip of this shaft is the only part of the clitoris that is visible from the outside. Anatomically speaking, it corresponds to the glans of the penis and is often described as being the size and shape of a pea. This tip is, in fact, what is generally known as “the clitoris”.
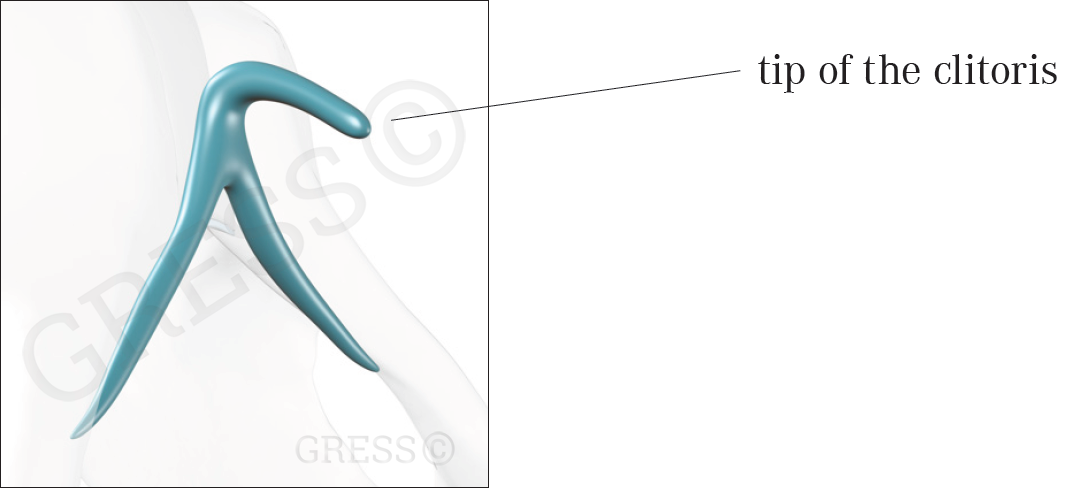
The clitoris consists of two arms combining to form a midline shaft. The tip of this shaft is the only visible part and is what is generally known as “the clitoris”.

Aesthetic and Functional Labiaplasty
ISBN 978-3-319-60222-6
International textbook by Prof. Stefan Gress, published by SPRINGER in January 2018.
go to book published by SPRINGER ...
CORRECTION OF A PROTRUDING CLITORIS (CLITORAL PROTRUSION)
The inner vaginal lips (labia minora) and the clitoris are completely different structures anatomically However, they are closely related topographically, as the labia minora flow closely around the clitoris on both sides.
If the labia minora are very long and very pronounced, the tip of the clitoris often sticks out a long way. We do not know why this happens. At first glance it is often not easy to see, as afterwards the tip of the clitoris is covered by the too-long labia minora and the large clitoral hood.
If the clitoral hood is tightened and the labia reduced (see composite reduction labiaplasty), a protruding clitoris may be more obvious than it was before, as the clitoris is not surrounded so much by the labia minora. It therefore makes sense, from both the aesthetic and functional points of view, to correct the clitoral protrusion, especially when it is desirable for the labia majora to cover the labia minora completely.
Example of enlarged labia minora with a large clitoral hood and protruding clitoris (clitoris protrusion)
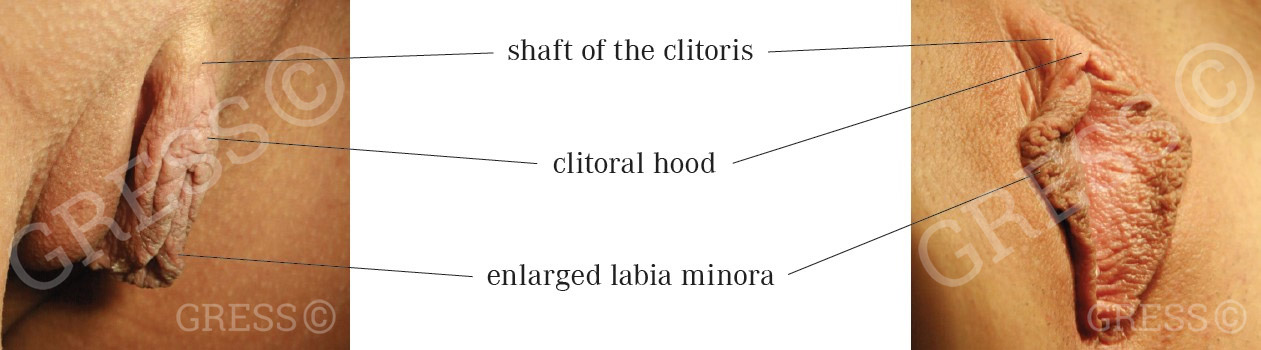
Diagram of the clitoris, showing the lateral view

How does it work?
You can’t just push a protruding clitoral tip back in, but it is possible to lower it. This involves simply removing a segment of skin below the clitoris and loosening the anchorage beneath. When the wound edges are brought together, the clitoris sinks in both the lateral and frontal planes.
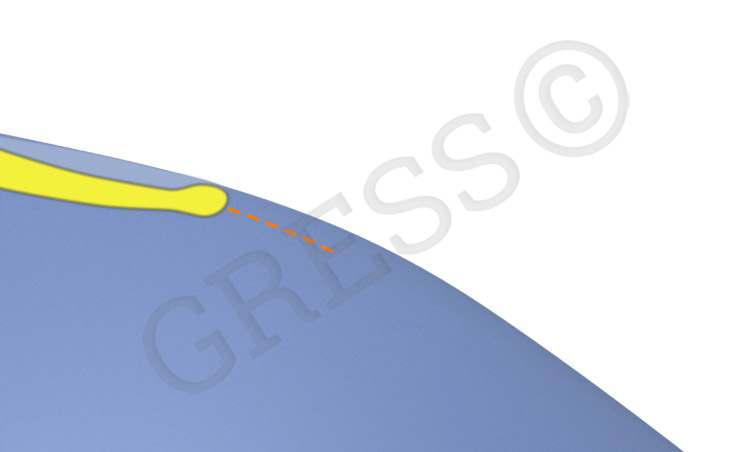
Diagrams showing how a protruding clitoris (clitoral protrusion) is corrected, lateral views
Clitoral protrusion:
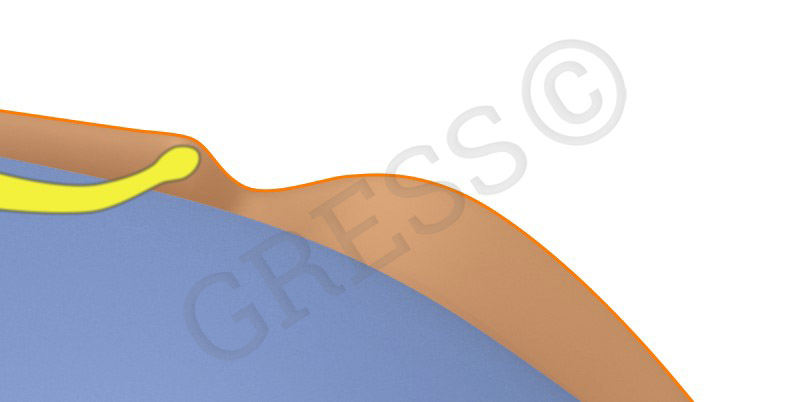
(clitoris: yellow, labia minora: orange, labia majora: blue)
Clitoral protrusion after reduction of the labia minora. The clitoris now visibly protrudes beyond the cover of the labia majora, lateral view.
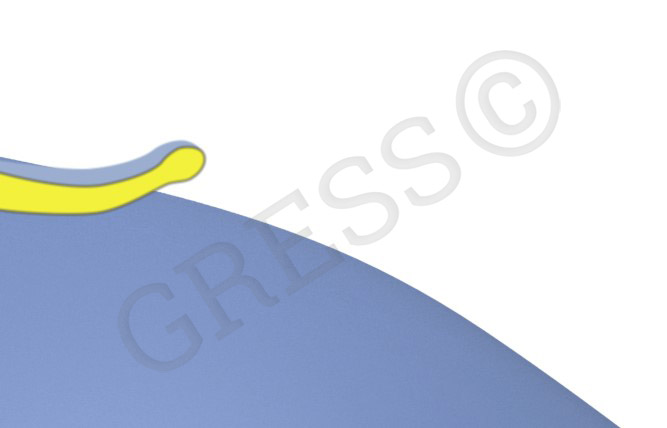
After the clitoris has been lowered, it is once again covered by the labia majora, lateral view.
As the clitoris itself is not touched during this procedure, there is no risk of loss of sensitivity. On the contrary, almost 40% of women find that the stimulation is better. This can be explained by the fact that the clitoris lies closer to the vaginal opening and can be stimulated directly.
For more information, go to composite reduction labiaplasty.
Correcting the position of the clitoris has become a fixed component of a composite reduction labiaplasty.
REDUCTION OF THE CLITORAL HOOD
The part of the labia minora that flows around the clitoris is known as the clitoral hood. It is not a separate anatomical structure, but part of the inner vaginal lips.
The clitoral hood varies considerably from woman to woman. It may be quite voluminous, covering the tip of the clitoris completely and hanging down like a curtain over it, or small and firm, leaving the tip of the clitoris partially or completely exposed.
Most patients want a firm clitoral hood that covers the clitoral tip fully or almost completely. A completely exposed clitoral tip does not mean any loss of sensitivity to sexual stimulation (the glans of the penis is also exposed in circumcised men), but many people find it more aesthetically pleasing when the clitoris is covered.
How is the clitoral hood tightened?
The techniques for labia minora reduction described here always include tightening of the clitoral hood (with the exception of variant 4). The technique of composite reduction labiaplasty offers a particularly effective means of tightening the clitoral hood. In addition to correcting clitoral protrusion, the clitoral hood is simultaneously tightened both above and below.
Learn more in the section on Labia minora reduction
CORRECTION OF TRUE CLITORAL ENLARGEMENT (HYPERPLASIA)
In a few cases there may be genuine enlargement of the clitoris itself. In this case, the entire clitoris is usually enlarged, not just the tip. The reasons for this are hormonal disturbances, especially during embryonic development, or masculinisation from taking hormones such as anabolic steroids for body building. Intersex conditions may also be present as the result of hormonal imbalance. The first essential step in treatment is to perform a comprehensive hormone analysis to identify the cause.
Technique
There are many procedures that can be used to alter the sexual organs, especially with intersex conditions, but we will not go into any detail here.
Reduction of a clitoral tip that is too large involves removing a wedge of tissue from the underside of the clitoral tip. When the edges of the wound are brought together, the size of the clitoral tip has been reduced by the volume of the tissue wedge that has been removed. No sensory loss is to be expected as the nerves supplying the tip run along the top of clitoris and the wedge is removed from underneath.
Frequently asked questions
Is the clitoris still covered?
As a rule, the clitoris is still covered by the clitoral hood as it was before the surgery. This question is asked very frequently, as women are concerned that the clitoris may lose its sensitivity if it is exposed. Even though this is not the case, we make sure that the covering is altered as little as possible and the situation remains the same as before.
Is loss of sensation a concern?
Neither the clitoris itself nor the relevant nerves are touched during the correction of clitoral protrusion or tightening of the clitoral hood. If the operation is performed correctly, there is no worry about any loss of sensitivity to sexual stimulation of the clitoris. As a rule, sensation remains as it was before the operation. In some cases (about 38%), sexual stimulation is even increased when the position of the clitoris has been corrected (e.g. following composite reduction labiaplasty), as the clitoris is located somewhat closer to the vaginal opening and can be stimulated more directly during sexual intercourse.
No sensory disturbances are to be expected with the reduction of true clitoral enlargement (hyperplasia), as the wedge that is removed comes from the underside of the clitoral tip, while the nerves radiate into the clitoris from above.
Can the clitoris be corrected without any reduction in the labia minora?
It is, of course, possible – but tightening up a very large or overhanging clitoral hood is always part of a labia minora reduction. The position of the clitoris is usually corrected together with a reduction labiaplasty. On the other hand, in the case of true clitoral hyperplasia, it is very possible to reduce the size of the clitoral tip without any associated correction of the labia.
Is it possible to correct the position of the clitoris purely to increase stimulation?
We do not really advise lowering the clitoris towards the vaginal opening purely for purposes of stimulation, as the chances of improving stimulation are quite low at 38%.
Aftercare
The operation will not affect your daily routine for very long. The first night after the operation is usually accompanied by a burning sensation and some pain, which will be perceived differently. However, this will have subsided significantly on the following day or might have disappeared altogether. From the third day onwards, you can have Sitz baths with camomile, and from the fourth day you can have a shower again. Please do not use any soap or shower gel for a week. You should wait for at least four weeks after the operation before you have intercourse again. The wounds will have healed, but can still be a little bit fragile. Before this time has elapsed, the wounds may reopen during strong mechanical exposure. As the scar is outside of the "area of friction", this does not affect intercourse in any way. Mechanical strains, which occur when exercising, or with sports like horse riding, cycling or jogging, are not recommended during the first four weeks. During the first two weeks after the operation, you should not use tampons, but sanitary pads during your menstrual period.
For more information on the preparation for surgery and postoperative care, please go to Information on reduction labiaplasty.









